
WiFi is the right fit when...
Cabling is impractical or cost-prohibitive to add.
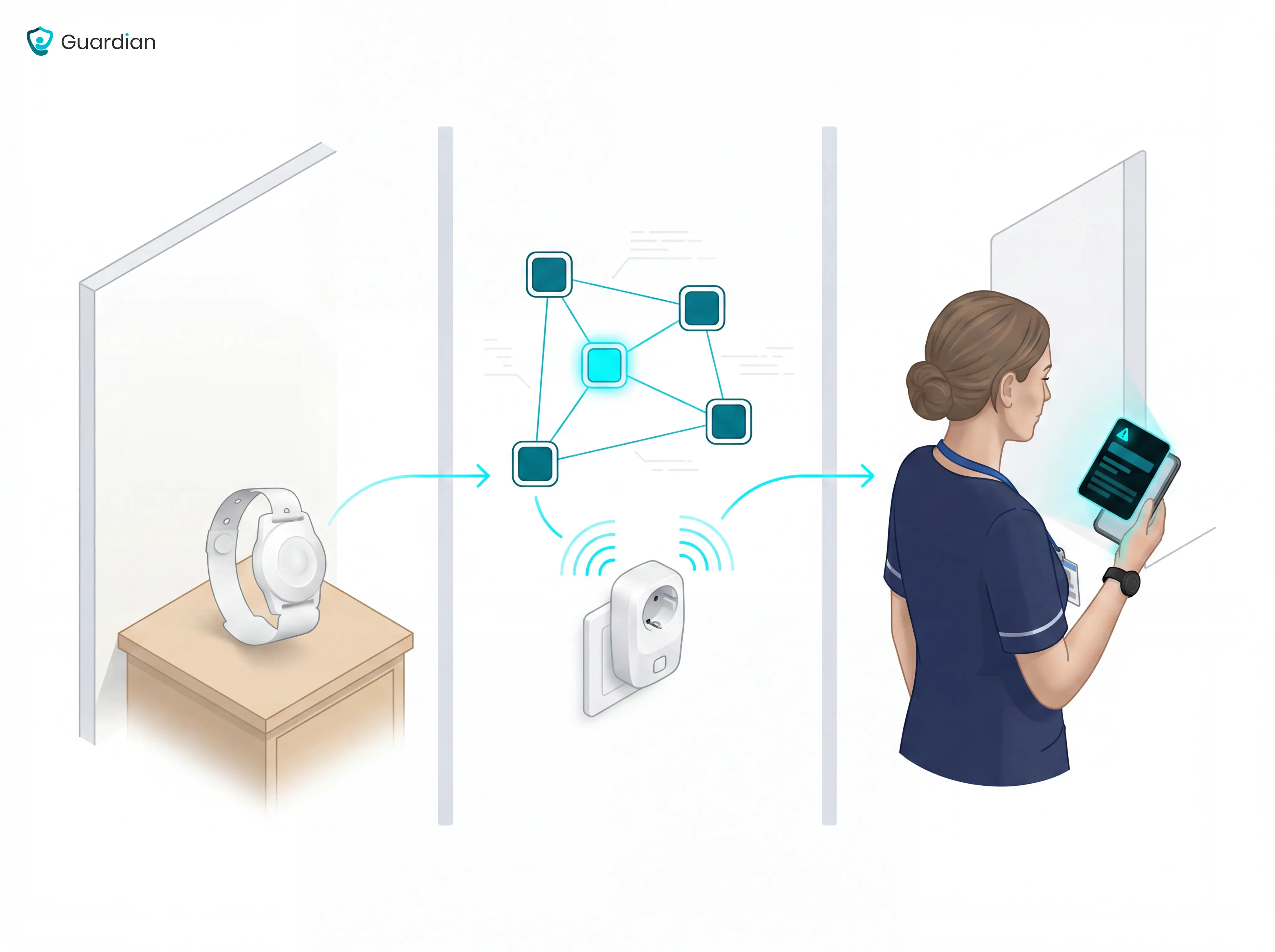
Staff need mobile app-based alerts on smartphones they already carry.
The facility has a reliable existing WiFi network.
Quick deployment on existing infrastructure is needed, with setup running about a week per ward.
Staff need mobile app-based alerts on smartphones they already carry.
The facility has a reliable existing WiFi network.
Quick deployment on existing infrastructure is needed, with setup running about a week per ward.




