26% of senior living executives name data privacy as their primary technology concern, driven by monitoring systems that process Protected Health Information.
Camera-based monitoring inside resident rooms is not accepted practice in UK and EU care settings, where GDPR and dignity standards apply.
Some facilities use cameras in communal areas with consent, but room-level camera monitoring is not permitted under standard regulatory frameworks.
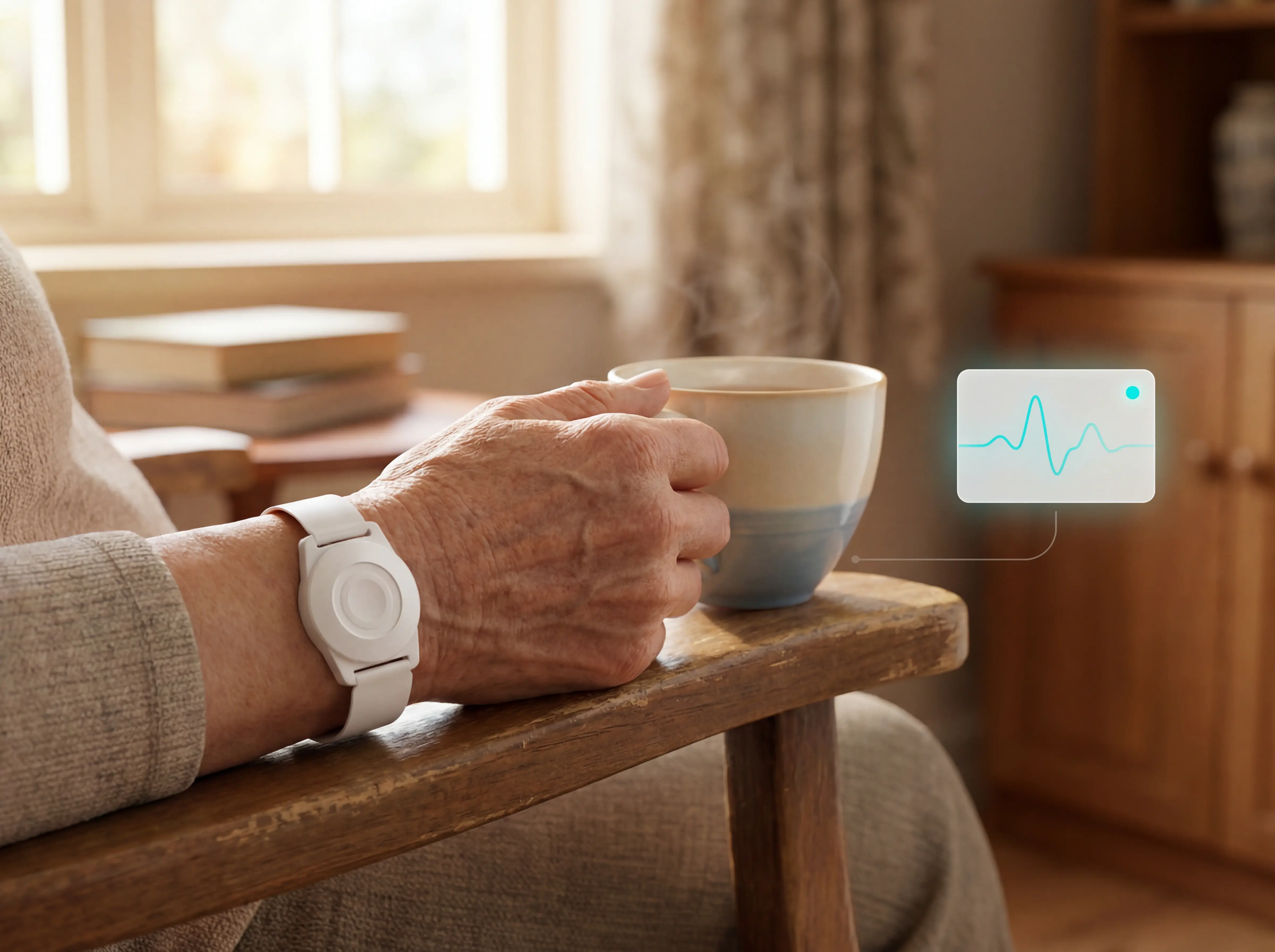
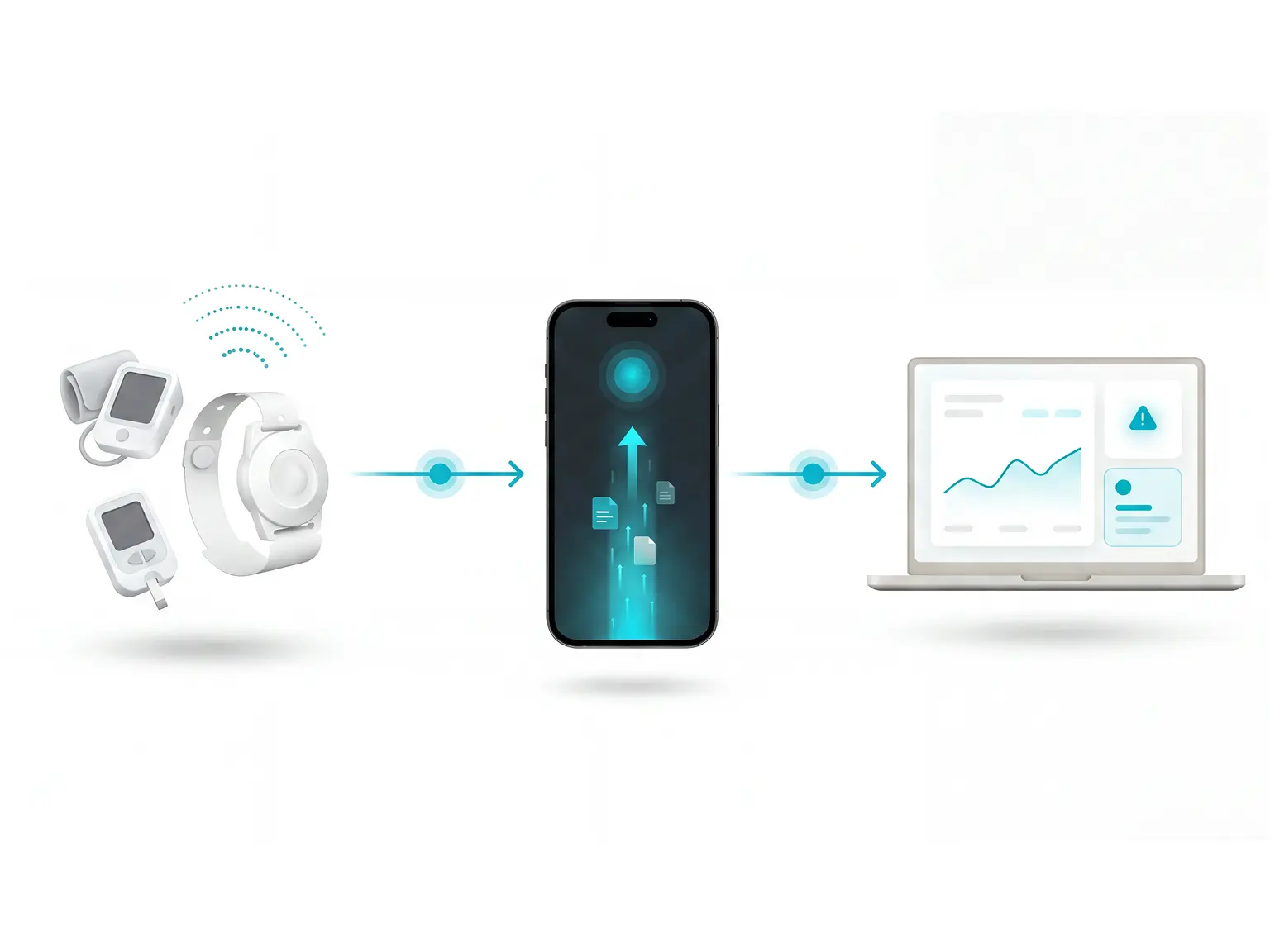
Senior emergency alert systems that do not capture images are the accepted alternative. Motion sensors, bed exit detectors, and door sensors provide the same safety signal without recording residents.
Confirm that any vendor you evaluate processes data in compliance with GDPR and your local regulatory framework before moving to a pilot.
In the EU, some RPM devices also fall under MDR 2017/745 classification requirements. Check whether your chosen hardware has CE marking under the correct risk class.